3.1.4 Total extraperitoneal repair (TEP)
With this procedure, the abdominal cavity is not opened. Hence, the risk of injury to internal organs, such as the intestines, is virtually zero. Via a small skin incision beneath the navel, a small balloon filled with air is inserted between the abdominal wall and peritoneum so as to separate these two layers from each other [Fig. 21]. The gap thus created is further enlarged by introducing carbon dioxide (CO2) for expansion of wall structures and better visibility [Fig. 22]. Via two other small skin incisions a working instrument and camera are introduced [Fig. 23 and Fig. 24]. The surgeon can now carefully expose the hernial sac and reposition the hernia contents in the abdominal cavity. A synthetic mesh is introduced via the hernia opening and, if necessary, this is further secured by means of a suture, tacks or tissue glue. But even without any fixation, the mesh rests firmly in place thanks to the naturally prevailing internal abdominal pressure [Fig. 25].
General anaesthesia is needed for endoscopic or minimally invasive surgery of inguinal hernias.
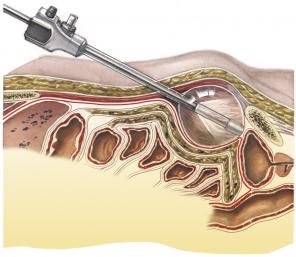
Fig. 21: Insertion of balloon (TEP)
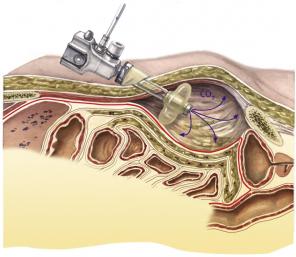
Fig. 22: Inflation with carbon dioxide (TEP)

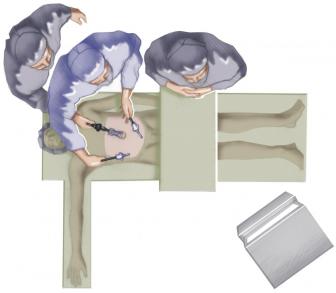
Fig. 23 and 24: Introduction of trocars (TEP)
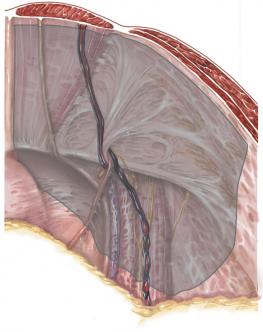
Fig. 25: Fitting synthetic mesh (TEP)